

By Kate Hawkins
Reports on the perils of antimicrobial resistance are becoming increasingly dire. Just this week the World Health Organization has warned that one in six bacterial infections is antibiotic-resistant. But this vulnerability and burden is not evenly distributed, low- and middle-income countries, with weak health systems are particularly affected. In affected countries some groups of people are more vulnerable and impacted than others. Global political shifts and slashed aid funding from richer countries place these countries at greater risk.
Another way is possible
A new paper in Nature Communications from the team at GEAR up, supported by the Fleming Fund, argues that current action on AMR fails to adequately address the social and political determinants that create vulnerability and the (gendered) power relations that keep inequity going. Much AMR research and policy frames AMR as a problem of antibiotic “misuse” and proposes solutions such as education and stronger regulation of the sale of antibiotics. Their critical interpretive synthesis of the knowledge points to the need to:
- Recognise interconnectedness: Of humans, the environment and animals
- Improve the evidence base on how gender roles, responsibilities and relationships contribute to AMR
- Consider the inequitable conditions of living and livelihoods associated with poverty and marginalisation and how these intersect with vulnerability
- Make the link between access to health services and country-level structural inequities and the relation to informal provision of antibiotics
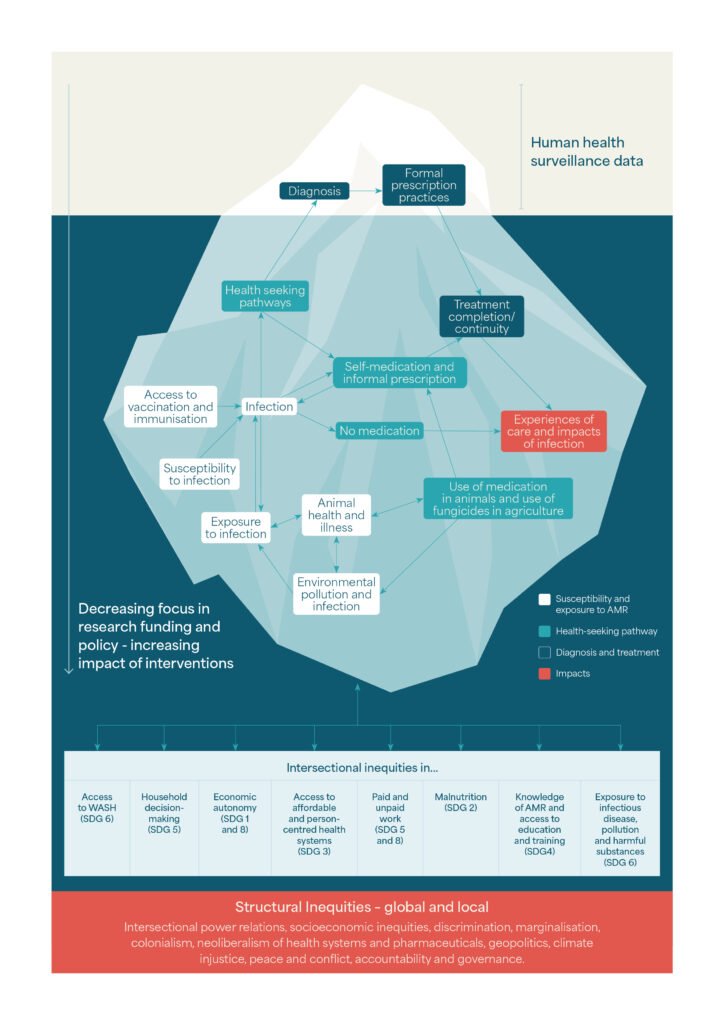
Introducing the iceberg
The paper uses the metaphor of the tip of the iceberg to show how a handful of interventions related to human health surveillance data collected at health centres are visible at the top. But where a myriad of issues lurk below. These reflect the complex reasons why people don’t access services or continue treatment.
Looking to the future
AMR is a “creeping disaster”, that requires integrated cross-sectoral and cross-border action and can only be addressed at the root. It is a matter of social justice. Future research should seek to address concerning evidence gaps around the underlying causes of inequities and injustices relating to AMR exposure, access to antimicrobials and lived experiences of AMR, with explicit attention to refugee and humanitarian contexts and those living in urban informal settlements. Attention to structural drivers requires multi-sectoral action and a focus on accountability, particularly for these populations particularly exposed or under-served by health systems. Research and action must also include the intersections of human health, animal health and environmental health, key dimensions of environmental and occupational justice and centre the voices of those most affected.
